Nevus of Ota (also known as "congenital melanosis bulbi", "nevus fuscoceruleus ophthalmomaxillaris", "oculodermal melanocytosis" and "Oculomucodermal melanocytosis") is a hyperpigmentation that occurs on the face as bluish/blue-to-gray speckled or mottled coalescing macules or patches within the distribution of the ophthalmic and maxillary branches of the trigeminal nerve (forehead, temple, zygomatic, or periorbital areas).
It is a hamartoma (from Greek hamartion “bodily defect”) of dermal melanocytes which have not migrated completely from the neural crest to the epidermis during the embryonic stage. But the true etiology and pathogenesis are unknown.
The color or perception of the color may vary to brown-violet, violet-blue, blue-green hues according to personal and environmental conditions (e.g. fatigue, menstruation, insomnia, cold or hot weather).
The nevus can be unilateral (one side of the face) or bilateral (in 5-10%.of cases), and, in addition to skin, it may involve parts of the eye (sclera, cornea, iris, retina) and inside of the mouth (oral mucosa).
It may be congenital (50% of cases present at birth) or acquired with the first peak of onset of nevus of Ota in infancy. The second peak of onset is seen during adolescence.
Nevus of Ota occurs most commonly in Asian population and more frequently in females. After onset, nevus of Ota may slowly and progressively enlarge and darken in color.
Its appearance usually remains stable once adulthood is reached. It was in 1939 that the condition was defined as an entity by Ota, from the University of Tokyo, who described bluish-gray irregular hyperpigmentation along the first and second divisions of the trigeminal nerve with frequent mucosal involvement as "Nevusfusco-caeruleus opthalmo-maxillaris and melanosis bulbi." Since then, this melanocytic nevus, which is common in Asians but rare in Caucasians, has been widely known as nevus of Ota.
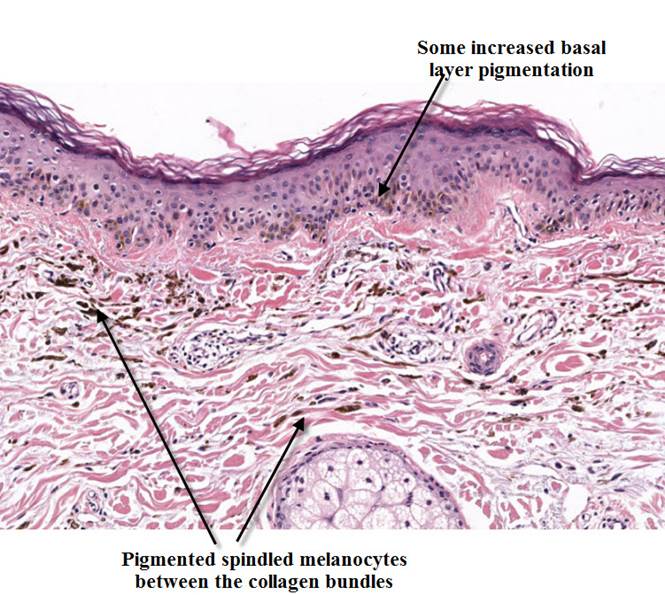
Although a diagnosis can usually be made without further investigation,skin biopsies are warranted if clinical changes are suspected of malignant transformation (eg, ulceration, new papular lesions, variegations in color) within the involved skin, ocular, or mucosal tissues. Usually nevus of Ota histologically show:
normal epidermis,
dendritic melanocytes surrounded by fibrous sheaths in the papillary and upper reticular dermis,
dermal melanophages
Nevi of Ota have been classified histologically into 5 types based on the locations of the dermal melanocytes (Hirayama and Suzuki, Dermatologica. 1991;183:169-172.):
superficial, when dermal melanocytes are located in the superficial layer of the dermis
superficial dominant, when dermal melanocytes have a diffuse distribution with a greater concentration in the superficial layer of the dermis
diffuse, when dermal melanocytes are evenly spread through the dermis
deep dominant, when dermal melanocytes have a diffuse distribution, but with a greater concentration in the deep layer
deep, when dermal melanocytes are located in the deep layer of the dermis
This histologic classification correlates clinically with the observation that the more superficial lesions tend to be located on the cheeks, while deeper lesions occur on periorbital areas, the temple, and forehead.
About treatment, because nevus of Ota can result in emotional and psychologic impact, the treatment is usually directed to cosmetic camouflage makeup to correct facial color changes.
But any unusual symptoms or changes to the lesional areas has to be referred to a physician, since a small risk for malignant degeneration exists.
Otherwise, laser treatment, with selective destruction of the dermal melanocytes, is the current treatment of choice.
If the eye is affected, it is not uncommon for patients with nevus of Ota to have ocular complications. Among the ocular complications, increased intraocular pressure with or without glaucoma was the most common (10%), followed by asymmetric cupping of the optic nerve head that was not associated with glaucoma, uveitis, cataracts and, rarely, orbital melanoma (0.5%).
Periodic ophthalmologic follow-up care is necessary to control intraocular pressure because of the risk of development of glaucoma.